von Willebrand’s Disease (vWD) is named after the Finnish doctor, Erik von Willebrand, who lived from 1870 to 1949. He was the first to describe vWD that he found in families in the Aland Islands. Although he could not identify the actual cause for the disorder, he was able to distinguish it from other bleeding disorders.
vWD is the most common type of bleeding disorder, affecting an estimated one percent of the world’s population. It affects females and males equally. However, because symptoms can be mild, many affected people have not been diagnosed or do not get diagnosed until later in life.
If you have vWD, you might be missing or have a deficiency of vWD factor (VWF). You might also have plenty of vWD factor, but it doesn’t function properly. This means that your blood cannot successfully form a clot or a platelet plug or because the site of the bleed cannot receive enough FVIII because the VWF doesn’t transport it properly. vWD is usually hereditary, but it can also be acquired. vWD heredity is very complicated. Acquired vWD is referred to as acquired von Willebrand Syndrome (aVWS).
People with vWD who have access to factor replacement therapy and other bleeding management medications have a normal life expectancy and are able to lead a fairly normal life. vWD is more frequently diagnosed in females because it causes menorrhagia in about 70% of cases; however, bleeding may decrease during pregnancy and childbirth due to hormonal changes raising levels of VWF and FVIII. In addition, it may be more severe in people with an ‘O’ blood type.
VWF has two roles in clotting:
- It makes platelets stick together to form a platelet plug.
- It ensures that there is enough FVIII in the bloodstream, binds to FVIII and carries it to the site of injury, and protects it from being broken down in the bloodstream.
Types of vWD
There are five types of vWD:
- vWD type 1
- vWD type 2
- vWD type 3
- Acquired or von Willebrand Syndrome (aVWS)
- Pseudo-vWD
vWD types 1 and 3 are quantitative, which means that if you have either of these types, you have a VWF deficiency. vWD type 2 is qualitative, which means that you might have enough VWF, but it doesn’t function properly, and it has several subtypes (in order of commonality: 2a, 2b, 2n, and 2m). Because each type and subtype of vWD has different treatments and therapies, it is important for you to know which type you have.
vWD type 2A used to be subclassified into types IIA, IIC, IID, and IIE, but discriminating between these subclassifications of type 2A did not show clinical utility, so they are all now referred to as type 2A.
vWD Type 1
vWD Type 1 is the most common (70% to 80% of those with vWD have this). If you have Type 1 vWD, your VWF works properly, but you do not have enough VWF in your bloodstream, which may challenge clotting ability and cause bleeding. Because VWF carries FVIII to the site of an injury, you may also have a low level of FVIII in your bloodstream. Many individuals with vWD type 1 are diagnosed late in life after a serious injury or a surgery.
vWD Type 2
vWD type 2 is the next most common (15% to 30% of those with vWD have one of the vWD type 2 subtypes). If you have vWD type 2, your vWF does not function properly, so even if you have plenty of it, you can still have bleeds. In order to understand vWD type 2, you need to know that the vWF protein has something called “multimers,” which bind it to platelets and FVIII. If the multimers are the wrong size or shape (or there aren’t enough of them), your VWF will not bind to platelets or FVIII, or it will bind at the wrong time. Since VWF is what stabilizes FVIII and carries it to the site of an injury, if this binding does not occur, either platelets do not get carried to the injury site to form a platelet plug, or FVIII does not get carried to the injury site to form a successful (fibrin) clot. (This can also cause circulating FVIII to be low, leading to a temporary misdiagnosis of hemophilia A.) The way each subtype of vWD type 2 malfunctions is a little different and may have different treatments and therapies that will work, so you need to know which subtype (2a, 2b, 2n, or 2m) you have:
Type 2a
If you have vWD type 2a, your VWF level is likely low, but the real problem is that you do not have enough large VWF multimers (cleaved multimers are too small and can’t cause adhesion) because they aren’t formed, which prevents your platelets from sticking together to make a good platelet plug.
Type 2b
If you have vWD type 2b, your VWF factor is likely low, but the real problem is that you do not have enough large VWF multimers because, after their secretion, they get bound to the platelets too soon (before an injury even happens). They then become cleaved, and the remaining cleaved multimers can’t bind to platelets. The body gets rid of the multimers that were bound to platelets too early, causing a shortage of both platelets and VWF in the blood, so you cannot form a platelet plug.
Type 2n
If you have vWD type 2n, your VWF works normally with platelets (so you will form the platelet plug), but it is not able to bind to FVIII and carry it to the site of an injury. Since VWF binding to FVIII is what stabilizes FVIII, you will also have low FVIII levels, challenging your ability to make a fibrin clot. (Due to the low FVIII caused by this, some individuals are temporarily misdiagnosed with mild hemophilia A.)
Type 2m
If you have VWD type 2m, you have approximately the right number of multimers, but your VWF is not able to bind to the platelets, so you cannot form a platelet plug.
vWD Type 3
If you have vWD type 3, you have the rarest type of vWD (about one person in a million) and usually the most severe symptoms. If you have vWD type 3, you have nearly undetectable or no VWF. Since VWF stabilizes and carries FVIII, you will also have low levels of FVIII. With low levels of both, you will not be able to form a platelet plug or a fibrin clot. This means that you can have spontaneous bleeding into your joints and muscles. In addition, you might have mucosal bleeds, such as nosebleeds, mouth bleeds, or menorrhagia. Due to the severity of symptoms, many are diagnosed with vWD type 3 at an early age.
Acquired vWD (aVWS)
If you have aVWS, you were not born with it. In fact, it occurs most often in individuals over 40 years of age with no prior bleeding history. aVWS usually occurs due to an additional disease state (e.g., tumor cell adhesion, and autoimmune response, or aortic stenosis).
Pseudo-vWD
If you have pseudo-vWD, also known as platelet-type vWD, your VWF levels are normal, your VWF is not defective, and your von Willebrand gene is not necessarily mutated. The real problem is actually with the platelet receptor, glycoprotein Ib (GPIb), in your blood that sometimes binds inactive platelets with VWF. These receptors are “over-active” and bind to the VWF too aggressively and too soon, so the body removes the bound platelet/VWF molecules, leaving you with potentially low platelet and VWF multimer levels.
Symptoms and Diagnosis
If you have vWD, you will likely bleed more often and for longer than someone who does not have a bleeding disorder. Anyone with any type of vWD can have the following symptoms:- Easy bruising
- Mucocutaneous bleeding
- Bleeding from the nose and gums
- Prolonged bleeding from cuts
- Menorrhagia (heavy or prolonged menstrual bleeding: longer than 5 days, more than 90 ml of bleeding, and/or clots larger than a grape)
- Bleeding may occur after surgery or when you have a tooth pulled
- Thrombocytopenia
- Blood in the urine
- Blood in the stools
- Hematomas
- Joint and muscle bleeds (usually vWD type 3)
- Gastrointestinal bleeding (usually vWD type 2A and aVWS)
Diagnosing vWD can be a complex process. Those who have milder vWD (usually vWD type 1 and vWD type 2) might not have any issues until later in life when a major injury or surgery occurs. Because vWD type 3 is so severe, diagnosis often occurs in infancy. Diagnosis also occurs earlier if there is a family history. Because VWF and FVIII levels shift with hormone changes, women especially should be screened more than once. For women, the best day to have your blood drawn and tested is on the first day of your menstrual cycle. In addition to a bleeding history, a coagulation study to diagnose vWD might include the following:
- FVIII coagulant activity
- Total blood count (assessing hemoglobin, hematocrit, platelet count [PC] and morphology, prothrombin time [PT], and activated partial thromboplastin time [aPTT])
- ABO blood group (those who have vWD and blood type O may have worse symptoms)
- Fibrinogen level thrombin time (TT)
- vWD profile testing
- VWF: Ag (plasma levels of VWF)
- VWF: RCo (function of VWF protein)
- FVIII: C (ability of VWF to carry FVIII)
- VWF multimer analysis
- VWF:CBA
- VWF:FVIIIB (specifically to diagnose vWD type 2n)
- RIPA (primarily to diagnose VWD type 2b, but may be an indicator for VWD type 3)
- Genetic testing (especially useful in differentiating vWD type 2n from hemophilia A)
- Platelet function analysis
Severity
vWD can be mild, moderate, or severe; however, severity is also tied to vWD type and blood type (because those with type O blood often have lower VWF levels). While there is an exception to every rule, in general, Types 1 and 2 vWD and pseudo-vWD tend to be mild or moderate. Type 3 vWD is severe. aVWS can range from mild to severe.Your treatment will depend on which type of vWD you have, your bleeding history, and any known bleeding patterns, so be sure you know which type/subtype you are and keep a log of known bleeds for reference. Treatment might involve factor replacement, hormonal therapy, or antifibrinolytics. Treatments and therapies are described below, divided by vWD type. Please note that VWF and FVIII replacement therapy can be in the same product, but each product has different ratios, so your hematologist will determine which product might work best for you.
vWD Type 1
- 1-desamino-8-D-arginine vasopressin (DDAVP)
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
vWD Type 2a
- DDAVP
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
vWD Type 2b
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics
vWD Type 2n
- VWF replacement therapy
- FVIII replacement therapy
- Hormonal therapy
- DDAVP (rarely works, but can be tried to find out)
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
vWD Type 2m
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
vWD Type 3
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
aVWS
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
- Topical bovine thrombin (topical and only for minor capillary bleeding)
- Fibrin sealant (only effective in certain surgical situations)
- Topical collagen sponges (useful for controlling bleeding wounds)
- Antifibrinolytics (clot stabilization)
Pseudo-vWD
- Hormonal therapy
- VWF replacement therapy
- FVIII replacement therapy
Topical bovine thrombin (topical and only for minor capillary bleeding) - Fibrin sealant (only effective in certain surgical situations)
Topical collagen sponges (useful for controlling bleeding wounds) - Antifibrinolytics (clot stabilization)
Inhibitors are extremely rare in vWD, but they occur in approximately 5–10% of people with vWD type 3. If you’ve developed an inhibitor, your body has developed antibodies (specifically, alloantibodies) against VWF, causing your body to reject treatment VWF, either by getting rid of it or (rarely) causing an anaphylactic reaction. You may be at higher risk for an inhibitor if you have a family history of inhibitors. There are no standard laboratory methods for identifying and characterizing antibodies for VWF, possibly because it’s so rare. However, some effective treatments exist, including recombinant FVIII, bypassing agents, and immune tolerance.
If you have inherited vWD, how you inherited it will depend on your vWD type. If you have a spontaneous mutation, your descendants will inherit vWD according to your type. In addition to the types listed below, one parent can have a genetic mutation, and the child can have a mutation as well, causing vWD.
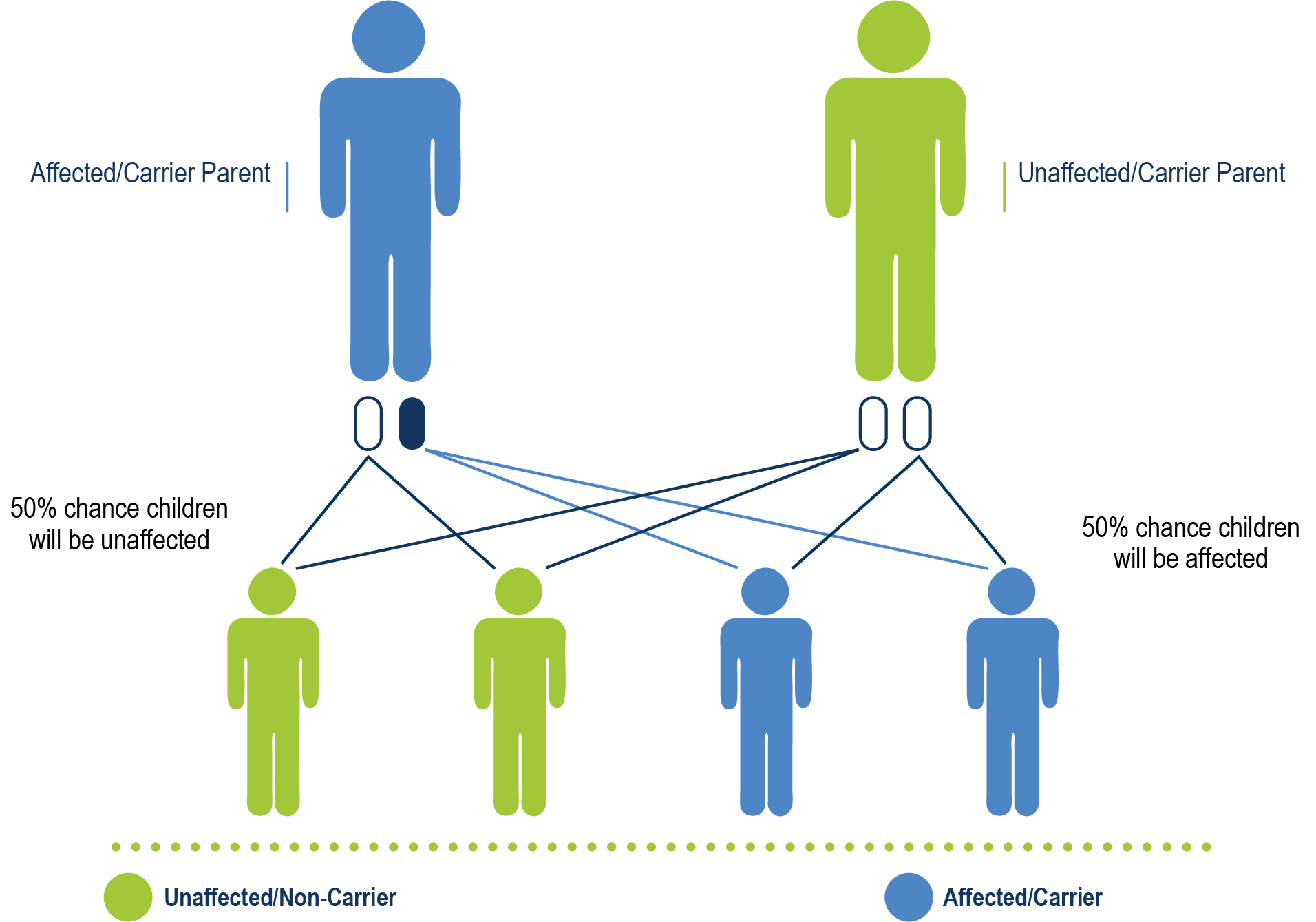
vWD type 1, vWD type 2 (all subtypes except 2n), and pseudo-vWD are all autosomal dominant. This means that even if only one parent has the mutated VWF gene, there is a chance of their children having vWD.
Autosomal Dominant Heredity
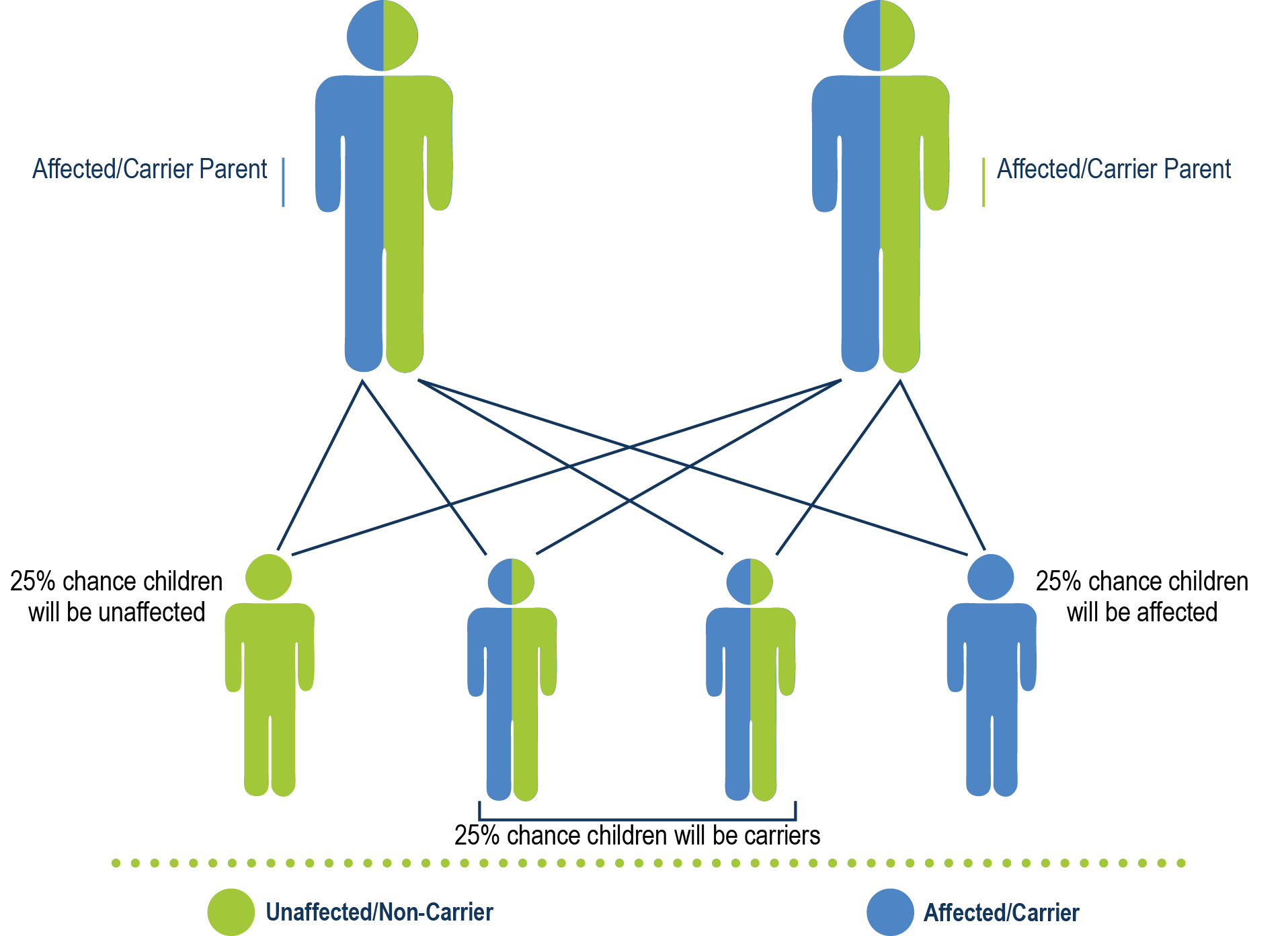
Autosomal Recessive Heredity
vWD type 3 and vWD type 2n are autosomal recessive. This means that both parents must have the defective VWF gene to create the possibility that their child will have vWD.